Basel, Switzerland (UroToday.com) Dr. Alberto Bossi spoke about the recommended treatment of men with pathological node-positive prostate cancer. These patients are becoming more common as surgery is being performed on a higher proportion of high-risk patients with positive nodes. Data presented at AUA 2018 by Bandini et al. from three referral centers in Italy, demonstrated that the rate of pathologically positive lymph node disease had increased from 5% in 1998 to 18% in 2016. This increase is due to both stage migration and the increased extent of pelvic lymph node dissection that has been performed through the years.
These patients are comprised of 3 distinct groups:
- Those with metastatic disease.
- Patient with Lymph node-positive prostate cancer.
- Patients with high risk localized and locally advanced prostate cancer.
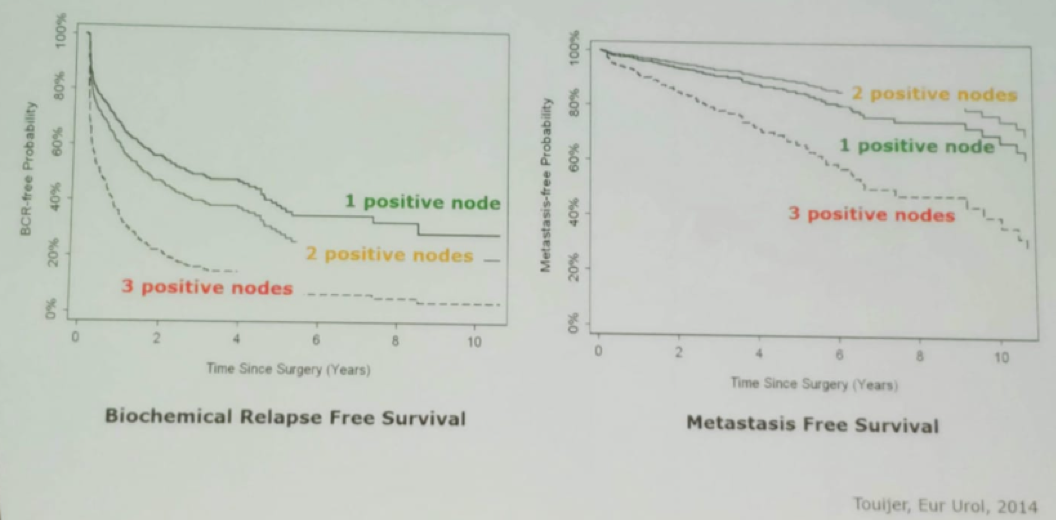
Several studies have assessed the local treatments that were given to patients with pathological positive nodes (Table 1). There is also data showing that the number of positive lymph nodes makes a difference in the final outcome of patients. Patients with one positive lymph node do better than patients with 2 and 3 positive lymph nodes in both metastasis-free survival and biochemical relapse-free survival (Figure 1).
Table 1- Local treatments to patients with pathological positive lymph nodes:
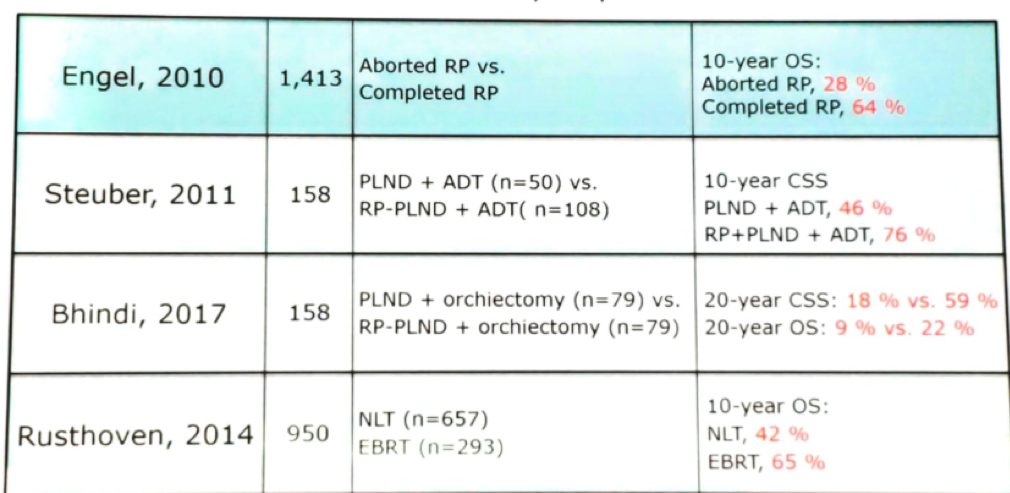
Figure 1 – Kaplan Meier curve showing that the number of positive lymph nodes affects final outcomes:
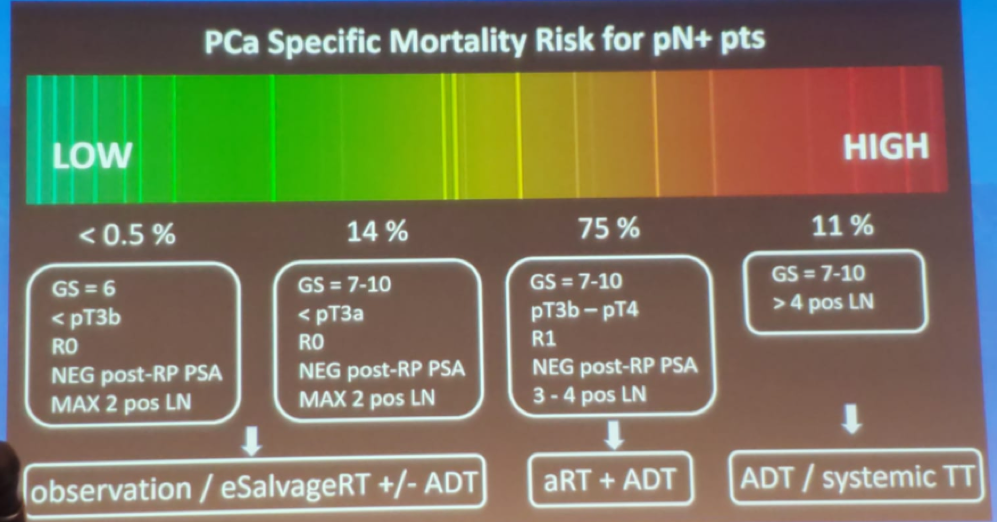
The prostate cancer-specific mortality risk for patients with positive pathological lymph nodes can vary from low to high risk, as demonstrated in Figure 2. While the low risk is not common, with approximately 14% of patients defined as low risk, their treatment could be limited to observation or early salvage radiotherapy +/- androgen deprivation therapy (ADT). In contrast, for high-risk patients, comprising approximately 11% of all patients, the treatment should be systemic with ADT and perhaps additional systemic targeted therapies. For the remaining bulk of patients, comprising 75% of all patients, the treatment should be adjuvant radiotherapy and the addition of ADT.
Figure 2 – Prostate cancer-specific mortality risk for patients with pathologically positive lymph nodes:
There are still many unanswered questions regarding the treatment of these patients following surgery. These include to which patients can we offer expectant management, whether we should always add ADT or is radiotherapy enough, and for the high-risk patients – what other systemic therapy should we add in addition to ADT.
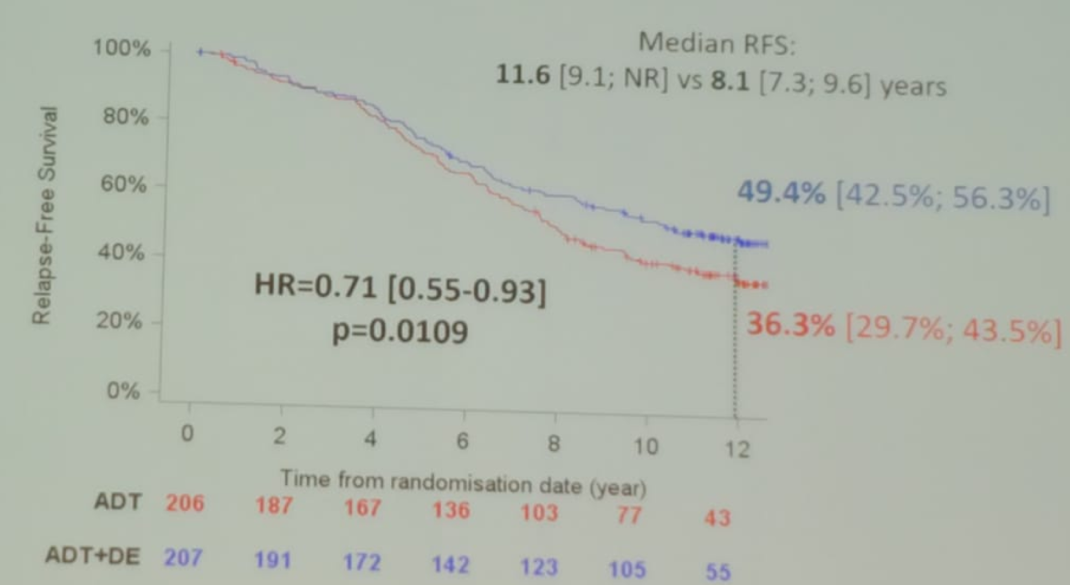
The GETUG-12 trial (Figure 3) helped us answer some of these questions as patients following surgery with high risk disease were randomized to either ADT for 3 years with the addition of docetaxel, or ADT alone with local treatment only. The accrual was between 2002 and 2006 with 413 patients included, and 29% of them being with pathological positive node disease. The results (Figure 4) demonstrated that ADT +docetaxel conferred a benefit in relapse-free survival, with an HR of 0.71, 95% CI 0.55-0.93, p=0.0109.
With the increasing number of high-risk patients being operated, we will be seeing more of these patients. Hopefully, we will be able to assess pertinent data in the near future, that will enable us to understand better how to treat these patients.
Figure 3- GETUG 12 TRIAL DESIGN:
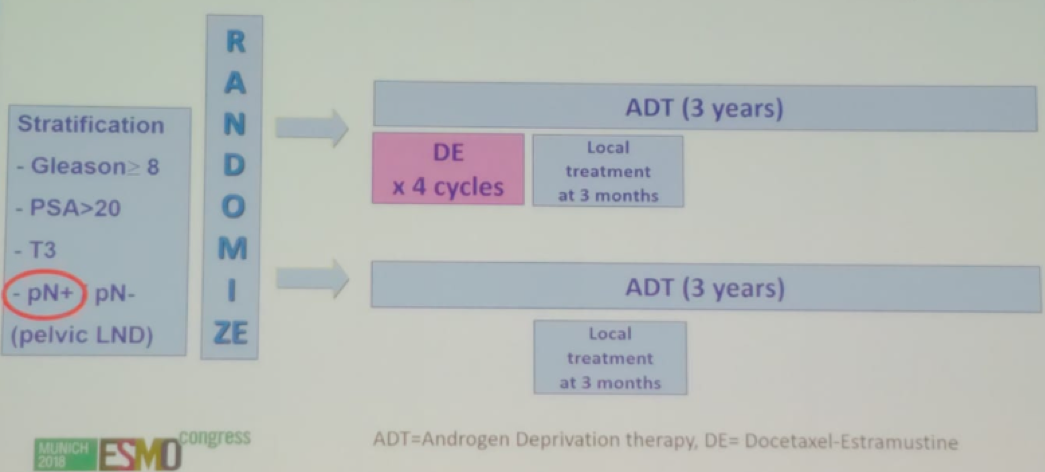
Figure 4 – GETUG 12 results:
Presented by: Alberto Bossi, MD, Head of the Urology and Prostate Brachytherapy Unit, Gustave Roussy Cancer Institute, Villejuif, France
Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, New-York, USA @GoldbergHanan at the 2019 Advanced Prostate Cancer Consensus Conference (APCCC) #APCCC19, Aug 29 – 31, 2019 in Basel, Switzerland